Intravitreal injections for
-
Diabetic macular edema.
-
Macular edema secondary to central retinal vein occlusion.
-
Macular edema secondary to branch retinal vein occlusion.
-
Subfoveal choroidal neovascularisation due to age related macular degeneration.
Why are intravitreal injections used?
Intravitreal injections deliver medication directly into the vitreous cavity of the eye. This allows high concentrations of treatment to reach the retina and macula, where swelling or abnormal blood vessel growth is affecting vision.
The medications most commonly used are anti-VEGF agents, which work by:
-
Reducing leakage from abnormal blood vessels
-
Decreasing retinal swelling (macular edema)
-
Suppressing abnormal new blood vessel growth
-
Diabetic Macular Edema (DME)
Why injections are needed
In diabetes, prolonged high blood sugar damages retinal blood vessels. These vessels become leaky, allowing fluid to accumulate in the macula, the part of the retina responsible for fine central vision.
Indications for treatment
-
Reduced vision due to macular edema
-
Retinal swelling involving or threatening the centre of the macula
-
OCT evidence of clinically significant macular edema
Treatment approach
-
Anti-VEGF injections are first-line therapy
-
Injections are typically started monthly until swelling improves
-
Laser or steroid treatments may be considered in selected cases
Goal
-
Reduce macular swelling
-
Stabilise or improve vision
-
Prevent long-term retinal damage
Macular Edema due to Retinal Vein Occlusion
(Central or Branch Retinal Vein Occlusion)


Why injections are needed
A retinal vein occlusion occurs when blood flow out of the retina is blocked. This leads to increased pressure, leakage, and fluid accumulation in the macula.
-
Central Retinal Vein Occlusion (CRVO): affects the main retinal vein
-
Branch Retinal Vein Occlusion (BRVO): affects a smaller retinal vein
Indications for treatment
-
Vision loss from macular edema
-
Persistent or worsening retinal swelling
-
OCT evidence of fluid involving the macula
Treatment approach
-
Anti-VEGF injections are the mainstay of treatment
-
Early treatment leads to better visual outcomes
-
Injection frequency depends on response and recurrence
Goal
-
Reduce macular edema
-
Improve or stabilise vision
-
Minimise long-term retinal damage
Subfoveal Choroidal Neovascularisation due to Age-Related Macular Degeneration (AMD)
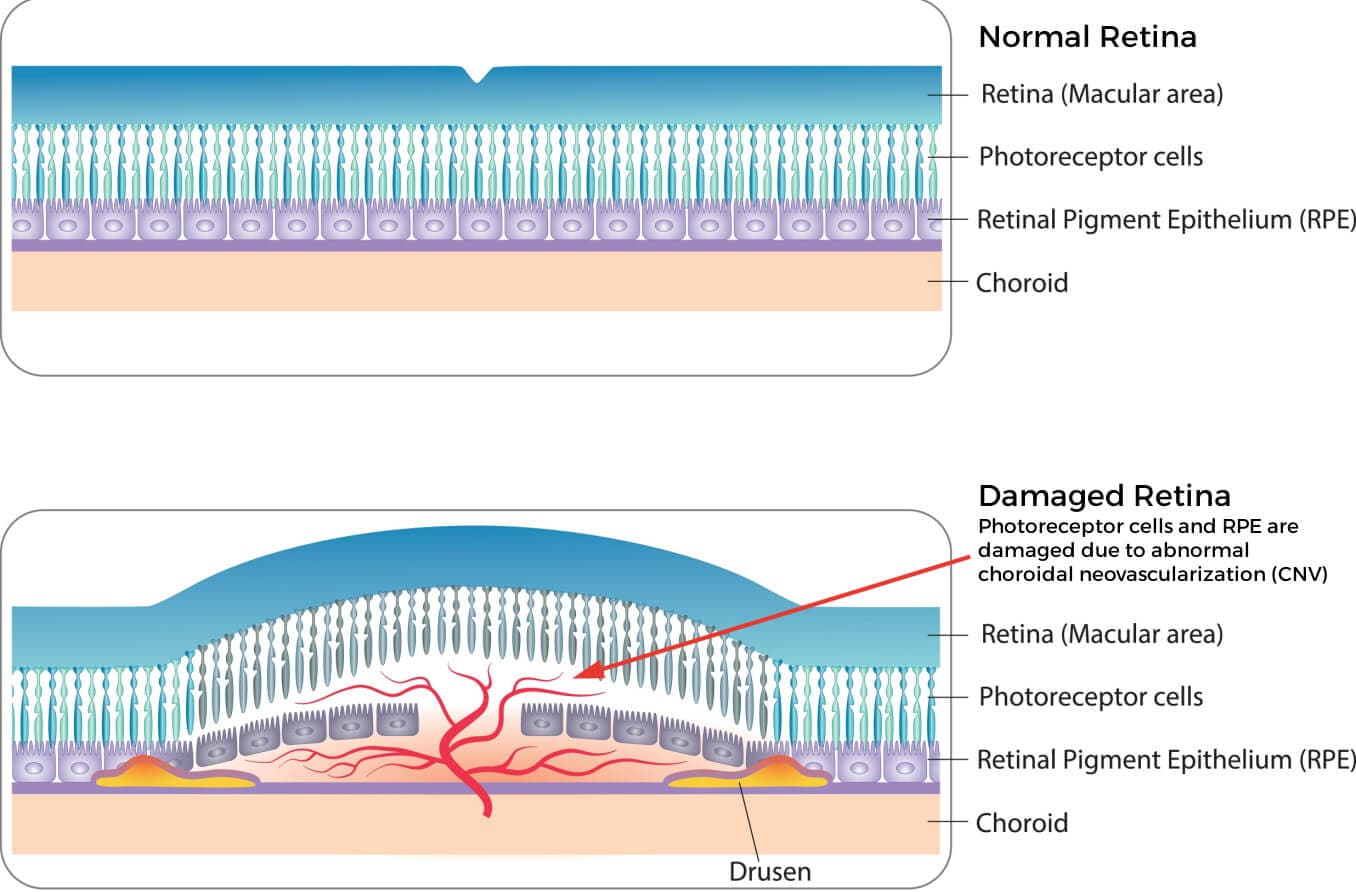

Why injections are needed
In “wet” AMD, abnormal blood vessels grow beneath the macula. These vessels leak fluid and blood, leading to rapid and potentially permanent central vision loss.
Indications for treatment
-
Distortion or loss of central vision
-
OCT or angiographic evidence of subfoveal neovascularisation
-
Active leakage or bleeding beneath the macula
Treatment approach
-
Anti-VEGF injections are essential and time-critical
-
Initial monthly injections are usually required
-
Long-term treatment is often necessary to maintain vision
Goal
-
Halt disease progression
-
Preserve central vision
-
Prevent irreversible scarring of the macula
Treat-and-Extend: General Treatment Principle
The treat-and-extend approach is commonly used for chronic retinal conditions.
How it works
- Loading phase
Injections are given regularly (often monthly) until the retina is dry and stable on imaging. - Extension phase
Once the retina is stable, injection intervals are gradually extended, usually by 2 weeks at a time
(e.g. from 4 weeks → 6 weeks → 8 weeks → 10 weeks → up to 12 weeks, depending on individual response). - Adjustment phase
If fluid or disease activity returns, the interval is shortened again to the last effective treatment interval.
Advantages
- Maintains disease control
- Reduces unnecessary injections
- Individualised to each patient’s response
Key point
Treatment is guided by retinal imaging and clinical response, not a fixed schedule.
Summary for Patients
-
Intravitreal injections are used to control swelling and abnormal blood vessel growth in the retina
-
They are vision-preserving treatments, not cures
-
Early and consistent treatment gives the best outcomes
-
Many patients require long-term monitoring and ongoing injections